
*Online Consultations Available
*Online Consultations Available
HTO | Opening Wedge | Closing Wedge | Tomofix
DFO | Double Level Osteotomy | Varus Correction
HTO + Cartilage | HTO + MAT | HTO + ACL/PLC
1,000+ Shoulder Surgeries performed
Rehab-Integrated
Care
Outcomes Tracked for 5 Years
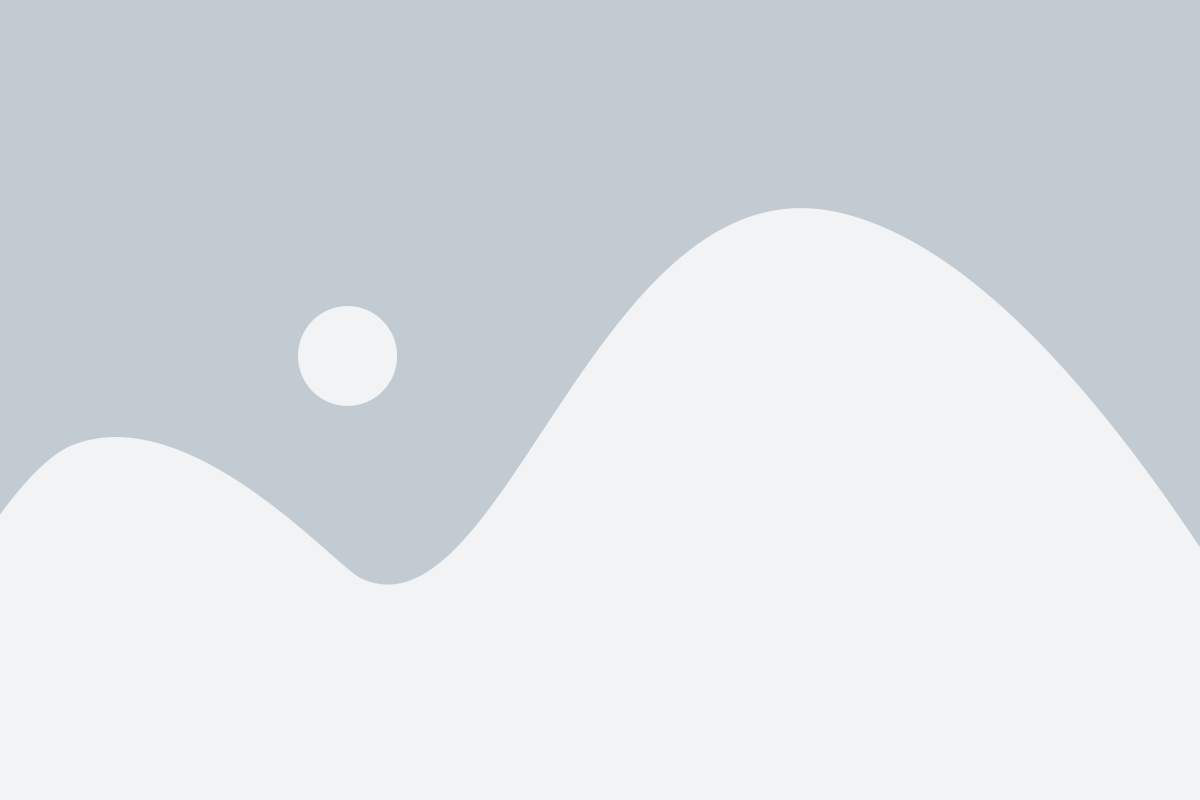
Varus knee malalignment — commonly called bow-legged alignment — occurs when the mechanical axis of the leg passes medial to (inside of) the center of the knee. The mechanical axis is the straight line from the center of the hip to the center of the ankle. In a normally aligned knee, this line passes through the center of the joint. In varus malalignment, it passes through the medial compartment — concentrating the body’s weight-bearing force on the inside of the knee.
The consequence of this alignment deviation is medial compartment overload: the cartilage, meniscus, and bone on the inside of the knee bear a disproportionate share of the load with every step. Over time, this overloading accelerates cartilage wear, meniscal damage, and early medial compartment arthritis — a predictable, mechanical outcome of an alignment problem.

A. Tibial varus:


Unlike any other condition in this series, varus knee malalignment requires a full-length standing alignment X-ray — taken from the hip to the ankle while bearing full weight — as the primary diagnostic and planning tool. A standard knee X-ray shows only the joint itself; a long leg alignment X-ray shows the entire mechanical axis of the limb.
Key measurements from the long leg standing X-ray:
MRI characterizes the secondary consequences of the chronic medial compartment overloading produced by varus malalignment. In patients with symptomatic varus, MRI typically shows:
The long leg X-ray and MRI characterize static varus deformity. The varus thrust — a dynamic finding assessed during walking — adds critical prognostic information. A varus thrust is a visible lateral displacement of the knee during the loading phase of gait: the knee thrusts outward with each step, reflecting dynamic instability superimposed on the static varus deformity.
Varus thrust is assessed clinically — by observing the patient walk — and on video analysis. A visible varus thrust is a surgically significant finding that indicates dynamic medial instability on top of the static deformity. Patients with varus thrust have a more aggressive disease trajectory and a stronger indication for early correction before the dynamic instability causes accelerated secondary damage.

*Same-day consultations may be available

A varus thrust is a dynamic gait abnormality in which the knee visibly shifts or thrusts outward during the loading phase of walking — the moment when body weight is transferred onto the leg. It is the dynamic expression of varus instability: the knee is not just statically bow-legged but mechanically unstable under load, producing a visible lateral thrust with each step.
Patients often describe this as: the knee feeling like it pushes outward when I walk, the knee bowing or buckling to the outside with each step, a visible worsening of the bow-legged appearance during walking compared to standing still, or a sensation of the knee giving outward rather than being reliably stable.

Conservative management for varus knee — bracing, injections, and physical therapy — addresses symptoms but does not correct the mechanical axis or stop progressive medial compartment damage.
For patients with early-to-moderate medial compartment damage in an otherwise preserved knee, TKR replaces a joint that still has significant structural value remaining.


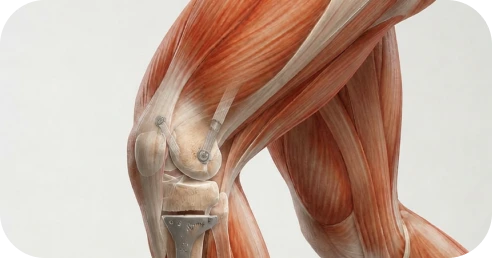
Osteotomy procedures for varus knee correction realign the mechanical axis of the leg by surgically cutting and repositioning the bone — shifting the weight-bearing line from the damaged medial compartment to a more neutral or slightly lateral position. The appropriate procedure depends on where the deformity originates (tibia, femur, or both), the magnitude of correction required, the concurrent pathology present, and patient factors including age and activity level.
High tibial osteotomy is the most commonly performed varus correction procedure and the primary indication for patients with tibial varus malalignment and medial compartment overloading. The proximal tibia — the top of the shin bone — is surgically cut and the bone is repositioned to shift the weight-bearing line from the medial compartment toward the lateral center of the knee.

A. Medial opening wedge HTO (most common):

B. Lateral closing wedge HTO:
The Tomofix plate is a locking angle-stable plate system specifically designed for opening wedge HTO fixation. Its angular stability allows early weight bearing without plate bending or deformation, reduces the biological demand on the bone graft fill, and provides reliable fixation throughout the healing period. The Tomofix plate and similar locked fixation systems have become the dominant fixation method for opening wedge HTO, replacing older wire and staple fixation techniques.
HTO correction is planned from the standing long leg X-ray. The target correction is to shift the weight-bearing line to approximately 62% of the tibial width — the Fujisawa point — which offloads the medial compartment while avoiding lateral compartment overloading. The planned correction determines the opening wedge angle and the expected post-operative mechanical axis.
When the varus deformity originates at the distal femur rather than the proximal tibia, distal femoral osteotomy corrects the alignment at the source of the deformity. DFO is less commonly performed than HTO because tibial varus is more prevalent, but is the appropriate correction for patients in whom the MPTA is normal and the deformity lies in the lateral distal femoral angle (LDFA).
When both the tibia and femur contribute to the overall varus deformity, correcting at a single level may require an overcorrection at that level that is biomechanically or technically inappropriate. Double level osteotomy addresses the tibia with HTO and the distal femur with DFO in a combined or staged approach.
Double level osteotomy is the most technically complex varus correction procedure and requires extensive pre-operative planning — including long leg X-ray analysis, CT-based planning in complex cases, and simulation of correction at both levels to determine the optimal combined correction. It is reserved for patients with significant combined tibial and femoral varus deformity.

Isolated HTO addresses the mechanical axis and offloads the medial compartment. But in many patients, the chronic medial overloading has produced concurrent damage to the cartilage, meniscus, or ligaments that must be addressed at the same time as the alignment correction. Correcting the alignment without addressing the concurrent pathology leaves structural problems that will continue to generate symptoms and degeneration.
When medial compartment cartilage damage has produced a focal defect — partial or full-thickness cartilage loss in an otherwise preserved medial compartment — concurrent cartilage restoration at the time of HTO addresses both the mechanical cause (alignment) and the structural consequence (cartilage defect). HTO shifts load away from the restored cartilage, creating the optimal mechanical environment for cartilage graft integration and healing.
Concurrent cartilage procedures: osteochondral allograft (OCA), ACI, MACI, OATS. The specific cartilage procedure depends on defect size, location, and the patient’s biology. See the Knee Cartilage and Joint Preservation page for procedure-specific details.

When the medial meniscus has been partially or completely removed in prior surgery — creating a meniscus-deficient knee — the varus knee is doubly at risk. The missing meniscus eliminates the primary shock absorber and stress distributor in the medial compartment, while the varus malalignment concentrates excessive force on that already-vulnerable compartment.
The combination of varus malalignment and meniscal deficiency is one of the strongest indications for combined HTO and meniscal allograft transplantation. MAT replaces the missing meniscus with a donor meniscal allograft matched to the patient’s anatomy. HTO simultaneously corrects the alignment to offload the transplanted meniscus and medial compartment. Performing HTO without MAT in a meniscus-deficient varus knee leaves the medial compartment vulnerable to ongoing accelerated deterioration despite the alignment correction.
Varus malalignment frequently coexists with ligamentous instability — particularly posterolateral corner (PLC) insufficiency, which contributes to varus thrust, and ACL deficiency, which is mechanically aggravated by varus malalignment. When ligament instability is present alongside varus malalignment, isolated osteotomy without ligament reconstruction — or isolated ligament reconstruction without alignment correction — produces unreliable results for both problems.
Combined HTO with concurrent or staged ACL reconstruction or PLC reconstruction addresses both the alignment and the instability simultaneously, creating the optimal mechanical environment for ligament graft function while correcting the deformity that would continue to stress the ligament.
One of the most common post-HTO procedures is plate and hardware removal — typically performed 12 to 18 months after the osteotomy, once bone healing is confirmed radiographically. The Tomofix plate and associated screws are removed as an outpatient procedure. Hardware removal is not always necessary, but is performed when the hardware is symptomatic — causing localized discomfort from the plate edge, hardware prominence, or patient preference for removal once healing is complete.
HTO is designed to delay rather than permanently prevent TKR. When an HTO has run its course — typically 10 to 15 years in well-selected patients — conversion to TKR is the appropriate next step. Prior HTO does not preclude TKR. In experienced hands, conversion TKR after prior HTO produces outcomes equivalent to primary TKR.
HTO recovery is governed by bone healing, not soft tissue healing — which distinguishes it from all other procedures in this series. The osteotomy site must heal as bone before the corrected alignment can be fully loaded. This produces a longer early recovery than ligament or tendon repairs, but a more durable long-term result once healing is complete.
Phase 1: Bone Healing and Protected Weight Bearing (Weeks 0-8)
Partial to toe-touch weight bearing with crutches, progressively increasing to full weight bearing as bone healing confirms on X-ray. The Tomofix plate provides immediate stability, allowing early protected weight bearing. Range-of-motion exercises begin immediately to prevent stiffness. Full weight bearing typically begins at 6 to 8 weeks when early healing is confirmed.
Phase 2: Rehabilitation and Strengthening (Weeks 8-20)
Progressive quadriceps and lower extremity strengthening as weight bearing normalizes. Functional movement training. Stationary bike and pool training when range of motion is adequate. Return to straight-line walking without assistive devices typically by 3 months.
Phase 3: Return to Sport and Activity (Months 4-9)
Return to lower-impact activities at 4 to 5 months. Running and cutting activities at 5 to 6 months for isolated HTO. Return to contact sport and heavy physical activity at 6 to 9 months. Combined HTO procedures (HTO + cartilage, HTO + MAT) extend recovery by 2 to 4 months depending on the concurrent procedure.

Drive?
Right leg surgery: typically 6 to 10 weeks when full weight bearing is achieved and off narcotics. Left leg: often 4 to 6 weeks.
Return to desk work?
Often 2 to 4 weeks with appropriate crutch mobility and leg elevation.
Return to lower-impact activity?
Cycling and swimming at 8 to 12 weeks.
Return to running?
Typically 5 to 6 months for isolated HTO.
Return to cutting sport or heavy physical work?
6 to 9 months for isolated HTO. 9 to 12 months for combined HTO procedures.
Weeks 0-2: Toe-touch weight bearing with crutches. Range of motion exercises immediately. Ice and elevation. Quad activation.
Weeks 2-6: Progressive weight bearing as tolerated. Crutches weaned when comfortable. Range of motion advancing.
Weeks 6-8: Full weight bearing confirmed by X-ray at 6-week check. Crutches discontinued.
Months 2-3: Normal walking without assistive devices. Progressive strengthening. Stationary bike.
Months 3-5: Progressive running program. Functional movement. Return to lower-impact sport.
Months 5-9: Return to cutting, pivoting, and high-demand activities. Plate removal at 12 to 18 months if indicated.
Modern arthroscopic repair techniques are associated with:
High rates of pain improvement
Significant gains in strength
Improved functional outcome scores
High patient satisfaction
1
We evaluate your mechanical axis deviation on long leg standing X-ray, characterize the medial compartment status on MRI, assess the lateral compartment and PF joint for preservation, evaluate for varus thrust on gait assessment, and determine whether the deformity is tibial (HTO), femoral (DFO), or combined (double level). We review concurrent pathology — cartilage, meniscus, ligament — to plan any required combined procedures.
2
We recommend the most appropriate correction procedure — HTO with opening or closing wedge, DFO, or double level osteotomy — and address the concurrent pathology plan: HTO + cartilage restoration, HTO + MAT for meniscus-deficient knees, or HTO + ligament reconstruction when instability coexists. We present the HTO vs. TKR positioning honestly for each patient’s specific anatomy and functional goals.
3
Our fellowship-trained shoulder surgeons perform
the planned osteotomy with Tomofix plate fixation, any required bone grafting, and concurrent procedures — cartilage restoration, meniscal allograft transplantation, ligament reconstruction — in a single surgical setting when feasible. Pre-operative correction planning from the long leg X-ray ensures that the target correction aligns with the Fujisawa point for optimal mechanical offloading.
4
Our surgeons work closely with physical therapists to implement the HTO-specific rehabilitation protocol — from protected weight bearing and range-of-motion recovery through progressive strengthening, functional training, and return-to-sport progression. Bone healing milestones on serial X-rays guide weight-bearing progression rather than calendar dates.
5
We track alignment maintenance on serial X-rays at 6 weeks, 3 months, 6 months, and 1 year, with continued monitoring at 2 and 5 years. Plate removal is planned at 12 to 18 months when indicated. Long-term surveillance ensures the correction is maintained and identifies any early progression that might alter the management plan.
This long-term follow-up monitors mechanical axis correction maintenance on serial X-rays, medial compartment pain resolution, return-to-sport rates by activity level, patient-reported quality-of-life measures, bone healing rates by technique (opening vs. closing wedge), plate removal rates and recovery, combined procedure outcomes (HTO + cartilage, HTO + MAT), and conversion-to-TKR rates and timing. These insights allow our surgeons to continually refine correction planning, combined procedure indications, and rehabilitation protocols to achieve the most durable alignment correction outcomes for each patient population.

1
Elite surgeons with decades of experience, incentivized to do the right thing
2
Prevent future surgeries
3
Heal with advanced, minimally invasive techniques
4
Preserve your natural joints, whenever possible
5
Seamless coordination from injury to recovery
6
Premium personalized care, made accessible
7
All patient outcomes tracked for 5 years
A high tibial osteotomy is a surgical procedure that corrects varus (bow-legged) malalignment at the proximal tibia by cutting the bone and repositioning it to shift the mechanical axis of the leg from the medial (inner) compartment toward a more neutral or slightly lateral position. The correction is stabilized with a plate and screws — most commonly the Tomofix plate — and the bone heals over 6 to 8 weeks in the corrected position.
For appropriate candidates — younger and middle-aged patients with tibial varus malalignment, preserved lateral compartment, and early-to-moderate medial compartment damage — HTO is a more biologically rational option than TKR. HTO preserves the native knee, corrects the mechanical cause of damage, and allows most patients to maintain an active lifestyle. Published 10-year outcomes show 70 to 85% of appropriately selected patients avoid TKR for at least 10 years. If and when TKR is eventually needed, prior HTO does not prevent it.
In opening wedge HTO, a wedge is opened on the medial side of the tibia and the gap is filled with bone graft, stabilized with a plate. In closing wedge HTO, a wedge of bone is removed from the lateral side and the bone is compressed closed. Both correct varus deformity reliably. Opening wedge (with Tomofix plate) is the dominant technique because it allows precise correction without requiring bone removal and preserves the fibula. The choice depends on the degree of correction needed and surgeon preference.
A varus thrust is a visible lateral displacement of the knee during walking — the knee thrusts outward with each step. It reflects dynamic instability superimposed on the static varus deformity and is a surgically significant finding. Patients with varus thrust have a more aggressive disease trajectory and a stronger surgical indication than patients with equivalent static varus but no thrust. A varus thrust cannot be corrected by bracing or physical therapy.
Yes. A standard knee X-ray shows only the joint. A long leg standing alignment X-ray — taken from the hip to the ankle while bearing full weight — shows the entire mechanical axis and is the gold standard for quantifying varus deformity and planning osteotomy correction. If you have not had a long leg standing X-ray, evaluation of your varus knee is incomplete for surgical planning purposes.
Yes — and in many patients this is the appropriate approach. When medial compartment cartilage damage or meniscal deficiency coexists with varus malalignment, isolated HTO without addressing the concurrent pathology leaves structural problems that continue to generate symptoms. Combined HTO with cartilage restoration (OCA, MACI, ACI) and HTO with meniscal allograft transplantation (MAT) are well-established combined procedures with documented outcomes. The combined approach is discussed at consultation based on your specific imaging findings.
The Joint Preservation Center accepts most PPO insurance plans that have out-of-network benefits:
If you have a PPO insurance plan with out-of-network benefits:
Note: If you have Medicare, Medicaid, TRICARE, or VA programs, or if your PPO does not have out-of-network benefits, you can still see our specialists and the surgery center will still be in-network. In this case, our specialists charge $250 for the initial office visit (all follow ups are included). Surgery is typically in the range of $6K – $8K depending on what you need done.
If you are unsure whether your plan is accepted, our team can verify your coverage before your appointment.
*Same-day consultations may be available
*Online Consultations Available