
*Online Consultations Available
*Online Consultations Available
1,000+ Shoulder Surgeries performed
Rehab-Integrated
Care
Outcomes Tracked for 5 Years

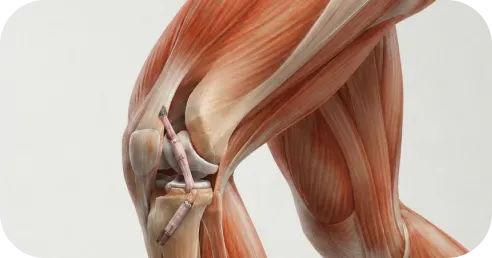
A. Grade 3 PCL tear with significant posterior instability



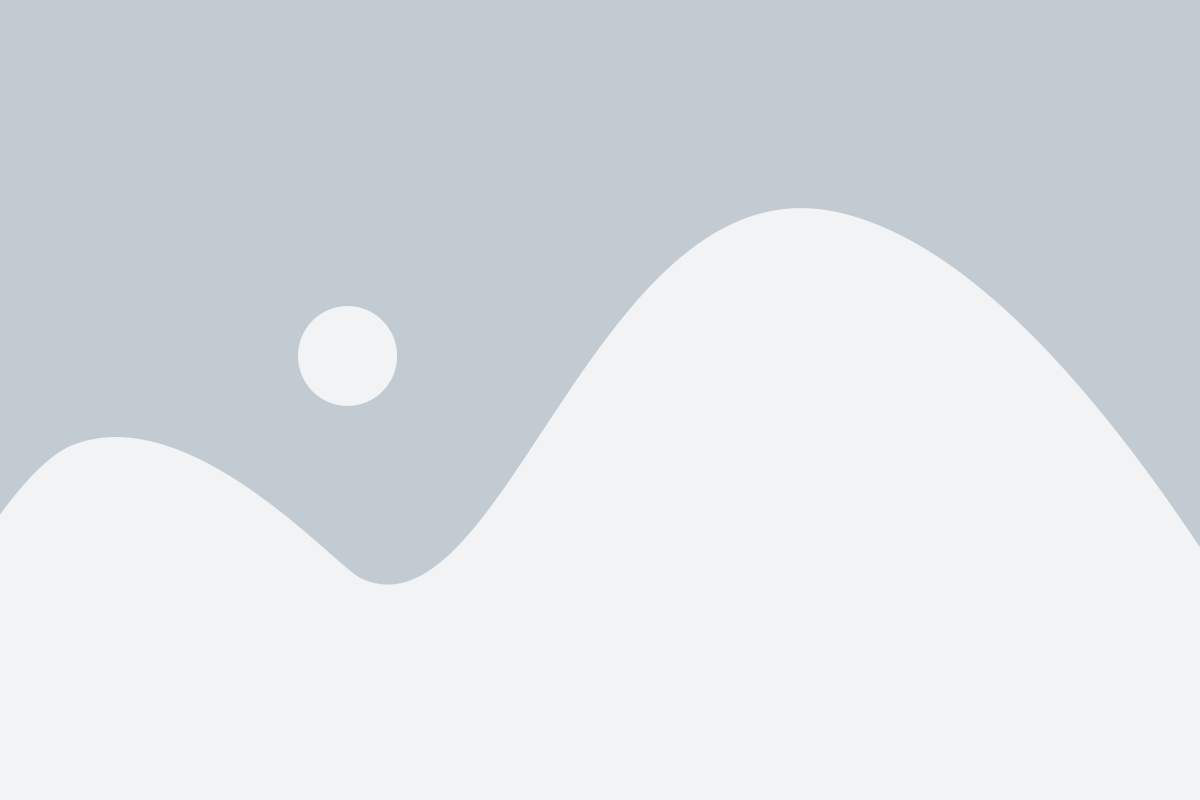
The posterior cruciate ligament (PCL) is the largest and strongest ligament in the knee. It connects the back of the tibia (the posterior tibial plateau) to the front of the femur (the medial femoral condyle), running diagonally through the interior of the knee. Its primary function is to prevent the tibia from sliding backward (posteriorly) relative to the femur — the opposite motion from what the ACL prevents.
The PCL is approximately twice as strong as the ACL. It is the primary reason that isolated Grade 1 and Grade 2 PCL tears often heal with conservative management — the ligament has sufficient residual tissue and vascularity to support functional healing in lower-grade injuries. Grade 3 tears with complete fiber disruption do not functionally heal, and the long-term consequences of untreated Grade 3 PCL deficiency are significant.
A. Grade 1
The posterior sag sign is the most pathognomonic clinical test for Grade 3 PCL tears. With the patient supine and the knee flexed to 90 degrees, the tibia visibly sags posteriorly (drops back) relative to the femur under gravity when PCL support is lost. The sag sign is positive when this posterior displacement is visible or palpable — the tibial tubercle falls behind the femoral condyles, reversing the normal slight anterior prominence of the tibia.
The posterior drawer test confirms posterior instability by manually pushing the tibia backward at 90 degrees of flexion. The degree of posterior drawer (in millimeters) corresponds to the PCL grade. On MRI, complete PCL fiber disruption confirms the clinical grade. Stress X-rays with posterior force applied measure the exact millimeters of posterior tibial translation and are the gold standard for objectively grading chronic PCL deficiency.

3-Tesla knee MRI with dedicated posterior cruciate sequences is the standard imaging for PCL injury. Key MRI findings:

A. PCL fiber signal and continuity

B. Associated PLC involvement

C. Associated ACL, MCL, and meniscal injuries

D. Posterior tibial avulsion
The PCL can avulse from its tibial insertion with a bone fragment rather than tearing within the ligament substance. A bony avulsion on MRI or CT may be amenable to direct screw fixation rather than ligament reconstruction — a favorable surgical situation.
Stress radiography — applying a posterior force to the tibia at 90 degrees of flexion and taking a lateral X-ray — measures the exact posterior tibial translation in millimeters bilaterally. This quantitative measurement is the gold standard for PCL grade assessment, particularly in chronic cases where clinical examination may be confounded by adaptive muscle guarding. Greater than 10mm asymmetric posterior translation is consistent with Grade 3 PCL deficiency.

*Same-day consultations may be available

PCL reconstruction replaces the torn posterior cruciate ligament with a tendon graft. It is indicated for Grade 3 tears in active patients with functional instability, all combined PCL injuries (PCL + PLC, PCL + ACL, PCL + MCL), and isolated PCL tears where conservative management has failed. The goal of reconstruction is to restore posterior tibial stability, eliminate the posterior sag, and prevent the secondary medial compartment and meniscal damage from chronic PCL laxity.

PCL reconstruction requires a large, strong graft — the PCL is the largest ligament in the knee and its graft must withstand significant forces. The graft choice depends on patient factors, activity level, and whether concurrent ligament reconstruction is planned.
The PCL has two functional bundles: the larger anterolateral (AL) bundle, which is taut in flexion, and the smaller posteromedial (PM) bundle, which is taut in extension. Single bundle reconstruction recreates the AL bundle — the primary restraint to posterior tibial translation. Double bundle reconstruction attempts to recreate both bundles, providing more complete stability across the full range of motion.

In a transtibial PCL reconstruction, the graft passes from the femoral tunnel through the posterior aspect of the tibia to exit at an acute angle — the so-called ‘killer turn’ at the posterior tibial tunnel entrance. This sharp graft angle creates localized stress concentration at the tibial tunnel lip, which can cause graft abrasion, elongation, or failure over time. The tibial inlay technique was developed specifically to eliminate this killer turn.
In the transtibial technique, a tibial tunnel is drilled from the anterior tibia, angling posteriorly to emerge at the PCL’s tibial insertion. The graft is passed through this tunnel from front to back and then looped up to the femoral tunnel, creating the killer turn at the posterior tibial tunnel lip. The transtibial technique is arthroscopic and technically reproducible. Its historical limitation is the killer turn — which may cause graft elongation over time compared to the tibial inlay.
The tibial inlay technique places a bone block directly into a trough cut in the posterior tibial PCL insertion, secured with a screw. The graft exits the tibia in a straight line to the femoral tunnel — eliminating the killer turn entirely. The graft path is more anatomic, and there is no acute angle at the tibial attachment. The tibial inlay requires a small posterior incision in addition to the arthroscopic portion of the surgery.
At consultation, we discuss which technique is most appropriate for your injury pattern, the planned concurrent procedures, and the specific graft selected.
A. PCL + PLC (Posterolateral Corner)

B. PCL + ACL

C. PCL + MCL

D. Knee dislocation with PCL and multiple ligaments
Chronic PCL deficiency — a PCL tear that was never repaired or that was managed conservatively — can remain functional for years before secondary damage produces increasingly limiting symptoms. The chronically PCL-deficient knee develops a compensatory muscular pattern that partially controls posterior instability — until progressive medial compartment cartilage loss, meniscal damage, or increasing functional demands overcome the compensation.
PCL reconstruction failure — when the knee remains unstable after surgery — has four primary causes, each requiring a different revision approach:
A second opinion with complete review of operative reports, current MRI, and clinical examination of all ligament systems — including the PLC — is essential before revision PCL surgery.

PCL reconstruction recovery is governed by the same graft ligamentization biology as ACL reconstruction — the graft is initially a passive scaffold that is progressively revascularized and remodeled into functional ligament tissue over 9 to 12 months. The PCL-specific consideration in early recovery is the gravity-driven posterior tibial sag: without muscular support, gravity pulls the tibia posteriorly when the knee is flexed and the muscles are relaxed. The early rehabilitation protocol specifically addresses this.
Unlike ACL rehabilitation where gravity does not directly stress the healing graft, PCL rehabilitation must account for the fact that gravity passively subluxes the tibia posteriorly when the hamstrings are relaxed and the knee is dependent. The early PCL protocol uses a specifically positioned brace that supports the tibia in a neutral or slightly anteriorly supported position — the tibial support position — to prevent gravity-driven posterior sag on the healing graft during the first 6 weeks.
Weeks 0-2: Knee brace with tibial support positioned to counteract posterior tibial sag. Partial weight-bearing with crutches. Quadriceps setting and straight-leg raises. Hamstring exercises are restricted — hamstring contraction produces posterior tibial force.
Weeks 2-6: Progressive weight-bearing. Range of motion progressing to 90 degrees. Quadriceps strengthening continues. No hamstring loading — the hamstrings are the primary posterior tibial force generator and protect against anterior tibial loading but actively stress the healing PCL graft.
Weeks 6-12: Full weight-bearing. Range of motion progressing toward full. Progressive quadriceps and hip strengthening. Hamstring loading cautiously introduced at 8 to 10 weeks under therapist supervision.
Months 3-6: Progressive strengthening. Proprioception and balance training. Cycling and swimming allowed. Jogging at 4 to 5 months.
Months 6-9: Progressive sport-specific training. Return to non-contact sport at 6 months.
Months 9-12: Return to contact sport with clearance based on functional testing.
When PCL and PLC are reconstructed simultaneously, the early recovery follows the PLC protocol — a hinged brace in valgus bias to protect the lateral structures — combined with the PCL tibial support position. Return to contact sport after combined PCL + PLC reconstruction typically extends to 10 to 14 months.
Drive?
Right leg surgery: typically 8 to 10 weeks. Left leg: often 4 to 6 weeks.
Return to desk work?
Usually within 2 to 4 weeks.
Return to light gym work?
3 to 4 months (upper body sooner).
Return to sport (non-contact)?
6 to 8 months.
Return to contact sport?
9 to 12 months for isolated PCL. 10 to 14 months for combined PCL + PLC.
Modern arthroscopic repair techniques are associated with:
High rates of pain improvement
Significant gains in strength
Improved functional outcome scores
High patient satisfaction
1
For acute PCL injuries, same-day evaluations are available. We perform the posterior sag sign test and posterior drawer test; assess for concurrent PLC involvement with the dial test; review your MRI for PCL grade, associated PLC or cruciate injuries, and tibial avulsion pattern; and determine whether the injury is isolated or combined and whether conservative management or reconstruction is indicated.
2
Unlike ACL, the PCL surgical decision requires individualized discussion. We clearly explain the surgical threshold — Grade 3 tears with instability in active patients, all combined injuries, and failed conservative management — versus the conservative indications. For patients with isolated Grade 2-3 tears who are considering conservative management, we discuss the long-term secondary damage risk transparently.
3
Our fellowship-trained shoulder surgeons perform the appropriate procedure — transtibial or tibial inlay reconstruction with Achilles allograft, hamstring autograft, or quadriceps autograft; single bundle or double bundle depending on injury pattern; combined PCL + PLC reconstruction when PLC involvement is confirmed — with the specific goal of eliminating posterior tibial sag and restoring full posterior stability.
4
Our surgeons work closely with physical therapists trained in PCL-specific rehabilitation — specifically the tibial support bracing position, the hamstring-avoidance protocol in early recovery, and the progressive quadriceps loading that is the primary mechanical basis for PCL rehabilitation. We coordinate directly with your physical therapist to ensure the PCL protocol is understood.
5
Return to contact sport clearance is based on posterior stability testing (stress X-ray normalization), strength symmetry testing, and functional movement assessment — not calendar dates alone. For chronic PCL deficiency patients, we perform serial medial compartment cartilage assessment to monitor for secondary damage progression and adjust the reconstruction timing accordingly.
This long-term follow-up monitors posterior tibial translation restoration (stress X-ray normalization at 6 months and 1 year), posterior sag sign resolution, return-to-sport rates and timelines by procedure type, graft failure and revision rates, combined PCL + PLC reconstruction outcomes versus isolated PCL outcomes, secondary medial compartment articular cartilage progression in chronic PCL deficiency patients, and patient-reported functional scores including going-downstairs stability. These data allow continuous improvement in graft selection, technique, and rehabilitation protocols.

1
Elite surgeons with decades of experience, incentivized to do the right thing
2
Prevent future surgeries
3
Heal with advanced, minimally invasive techniques
4
Preserve your natural joints, whenever possible
5
Seamless coordination from injury to recovery
6
Premium personalized care, made accessible
7
All patient outcomes tracked for 5 years
No — PCL surgery is not always necessary, and this is one of the most important differences between PCL and ACL tears. Grade 1 and Grade 2 isolated PCL tears can often be managed successfully with physical therapy, quadriceps strengthening, and bracing in most patients. Grade 3 isolated tears in active adults with functional instability are surgical candidates, but even these can sometimes be managed conservatively in low-demand patients. The surgical threshold that is clear and absolute: PCL combined with PLC or other ligament injuries, and knee dislocations. For isolated Grade 3 tears, the decision requires individualized discussion based on activity level and functional demands.
A dashboard injury occurs when a force is applied to the front of the bent knee — as in a motor vehicle collision where the knee strikes the dashboard. This impact drives the tibia backward (posteriorly) relative to the femur, tearing the PCL. The mechanism is a posterior-directed force, opposite to the anterior shear that tears the ACL. Any direct blow to the front of the tibia with the knee bent — from a tackle, fall, or occupational injury — produces the same mechanism. The PCL is the primary restraint to this posterior tibial translation.
Transtibial reconstruction drills a tunnel from the front of the tibia to the PCL insertion at the back, and the graft passes through this tunnel at an acute angle — the ‘killer turn’ at the posterior tibial tunnel lip. This sharp angle can cause graft stress over time. The tibial inlay technique places a bone block directly into the posterior tibia at the PCL insertion, eliminating the killer turn by creating a straight graft path. Tibial inlay is preferred when a posterior approach is already planned (as in combined PCL + PLC reconstruction) and may offer biomechanical advantages in graft durability.
The most common cause of PCL reconstruction failure is a missed concurrent PLC (posterolateral corner) injury that was not addressed at the time of initial surgery. The uncorrected PLC instability places the PCL graft under continued varus and rotational loads, causing progressive graft elongation or failure. Before revision PCL reconstruction, the entire lateral and posterolateral complex — LCL, popliteus tendon, and PFL — must be evaluated on MRI and clinical examination. Revision surgery almost always requires combined PCL + PLC reconstruction when the PLC was previously missed.
The posterior sag sign is the most pathognomonic physical examination finding for a Grade 3 PCL tear. With the patient lying on their back and the knee bent to 90 degrees, gravity pulls the tibia backward — causing the tibia to visibly ‘sag’ posteriorly relative to the femur. In a normal knee, the tibial tubercle sits slightly anterior to the femoral condyles at 90 degrees. In a Grade 3 PCL tear, the sag reverses this relationship — the tibia drops back behind its normal position. The posterior sag sign is present because the PCL normally prevents this gravity-driven posterior tibial translation.
The Joint Preservation Center accepts most PPO insurance plans that have out-of-network benefits:
If you have a PPO insurance plan with out-of-network benefits:
Note: If you have Medicare, Medicaid, TRICARE, or VA programs, or if your PPO does not have out-of-network benefits, you can still see our specialists and the surgery center will still be in-network. In this case, our specialists charge $250 for the initial office visit (all follow ups are included). Surgery is typically in the range of $6K – $8K depending on what you need done.
If you are unsure whether your plan is accepted, our team can verify your coverage before your appointment.
*Same-day consultations may be available
*Online Consultations Available